


 Sign Out
Sign Out



Clinical experience - dapagliflozin: Two major pools of patients were used to evaluate adverse effects with dapagliflozin 10 mg versus control; a pool of 13 placebo-controlled studies and a larger pool comprised of 21 active- and placebo-controlled studies. In addition, dapagliflozin has been studied in patients with heart failure with reduced ejection fraction and in patients with chronic kidney disease.
In the dedicated cardiovascular outcomes study in patients with type 2 diabetes mellitus (DECLARE), 8574 patients received dapagliflozin 10 mg and 8569 received placebo for a median exposure time of 48 months. In total, there were 30623 patient-years of exposure to dapagliflozin.
Placebo-controlled studies: The first pool is a pre-specified pool of patients from 13 short-term, placebo-controlled studies including the monotherapy studies, add-on studies, and the initial combination with metformin study. In the pool, 2360 patients were treated with dapagliflozin 10 mg and 2295 were treated with placebo with a mean duration of exposure of 22 weeks.
The overall incidence of adverse events in patients treated with dapagliflozin 10 mg was 60.0% compared to 55.7% for the placebo group. The incidence of discontinuation of therapy due to adverse events in patients who received dapagliflozin 10 mg was 4.3% compared to 3.6% for the placebo group. The most commonly reported events leading to discontinuation in patients and reported in at least 3 dapagliflozin 10 mg treated patients were renal impairment (0.8%), decrease in creatinine clearance (0.6%), increased blood creatinine (0.3%), urinary tract infections (0.2%), and vulvovaginal mycotic infection (0.1%).
Active- and placebo-controlled studies: The second pool is a pool of patients from 21 active- and placebo-controlled studies used to evaluate and present data for malignancies and liver tests. In this pool, 5936 patients were treated with dapagliflozin and 3403 were treated with control (either as monotherapy or in combination with other antidiabetic therapies). These 21 studies provide a mean duration of exposure to dapagliflozin 10 mg of 55 weeks (6247 patient-years).
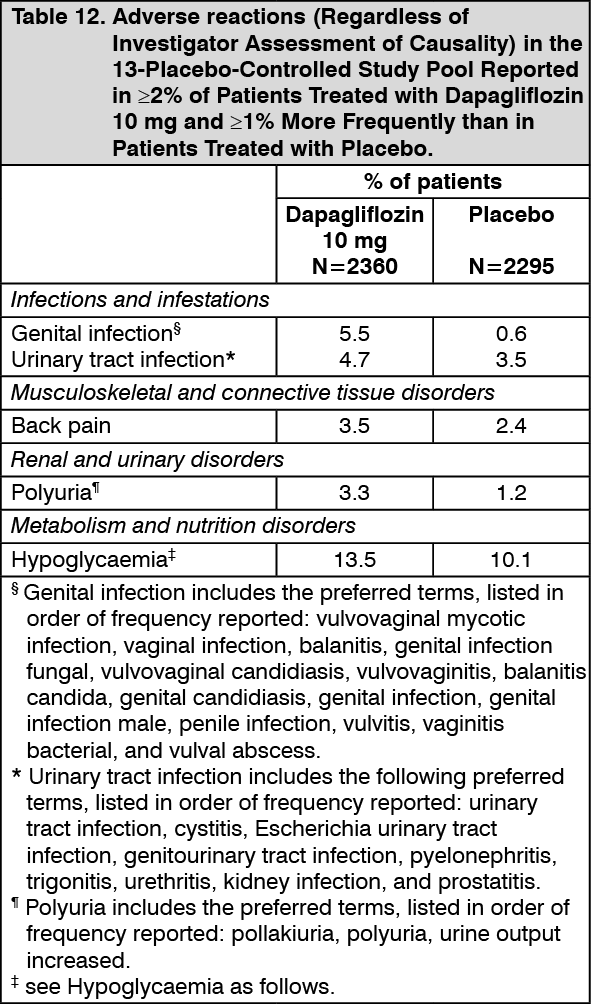
The adverse events in the 13-study placebo controlled pool reported (regardless of investigator assessment of causality) in ≥2% of patients treated with dapagliflozin 10 mg and ≥1% more and at least 3 patients more than treated with placebo are shown in Table 12. (See Table 12.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdditional adverse reactions in ≥5% of patients treated with dapagliflozin 10 mg, ≥1% more than patients in placebo/comparator, and reported in at least three more patients treated with dapagliflozin 10 mg and regardless of relationship to dapagliflozin reported by investigator, are described as follows by treatment regimen.
In the add-on to metformin studies: headache (5.3% dapagliflozin 10 mg and 3.1% placebo).
Diabetic ketoacidosis was identified with a frequency of rare (≥1/10,000 to <1/1000), based on annual rate, in a large cardiovascular outcomes study with dapagliflozin in patients with type 2 diabetes.
Description of selected adverse events: Hypoglycaemia: The frequency of hypoglycaemia depended on the type of background therapy used in each study. Studies with add-on sulfonylurea and add-on insulin therapies had higher rates of hypoglycaemia with dapagliflozin treatment than with placebo treatment (see Precautions).
In studies of dapagliflozin in initial combination therapy with metformin, add-on to metformin alone up to 102 weeks there were no major episodes of hypoglycaemia reported. In a study of dapagliflozin added on to sitagliptin (with or without metformin) for up to 48 weeks, one major episode of hypoglycaemia was reported in a patient treated with dapagliflozin 10 mg plus sitagliptin (without metformin). In these studies, the frequency of minor episodes of hypoglycaemia was similar (<5%) between treatment groups, including placebo.
In a study with dapagliflozin 10 mg added on to glimepiride for up to 48 weeks, that also included other doses of dapagliflozin, one episode of major hypoglycaemia in a patient in the dapagliflozin 2.5 mg plus glimepiride group was reported. Minor episodes of hypoglycaemia were reported in 7.9% patients in the dapagliflozin 10 mg plus glimepiride group and 2.1% patients in the placebo plus glimepiride group.
In an add-on to metformin study that compared dapagliflozin to glipizide up to 104 weeks, there were 3 episodes of major hypoglycaemia in the glipizide plus metformin group and none in the dapagliflozin plus metformin group. Minor episodes of hypoglycaemia were reported in 2.5% of patients in the dapagliflozin plus metformin group and 42.4% of patients in the glipizide plus metformin group.
In an add-on to metformin and a sulfonylurea study, up to 52 weeks, no episodes of major hypoglycaemia were reported. Minor episodes of hypoglycaemia were reported in 15.6% of subjects who received dapagliflozin 10 mg plus metformin and a sulfonylurea and in 4.6% of subjects who received placebo plus metformin and a sulfonylurea.
In the analysis of pooled safety data of 1169 patients from trials evaluating saxagliptin in combination with dapagliflozin at 24 weeks, the overall incidence of hypoglycaemia for the pooled safety data of was low (≤1.8% in any treatment group); there was no increase in hypoglycaemia in saxagliptin plus dapagliflozin plus metformin treatment group compared to the saxagliptin plus metformin or dapagliflozin plus metformin treatment groups. The combined use of saxagliptin plus dapagliflozin plus metformin was not associated with an increase in the risk of hypoglycaemia when compared to the individual agents as monotherapy. This was consistent with prior clinical trial experience regardless of whether the combination was added to metformin concurrently or sequentially.
In a study of dapagliflozin 10 mg initiated concomitantly with extended release exenatide (on a background of metformin), there were no episodes of major or minor hypoglycaemia reported.
In an add-on to insulin study up to 24 weeks, episodes of major hypoglycaemia were reported in 1 (0.5%) patient in dapagliflozin 10 mg plus insulin and placebo plus insulin groups, respectively. Up to 104 weeks, 2 (1.0%) and 1 (0.5%) of patients in dapagliflozin 10 mg plus insulin and placebo plus insulin groups reported major episodes. Up to 24 weeks, minor episodes were reported in 79 (40.3%) patients in the dapagliflozin 10 mg plus insulin group and in 67 (34%) patients in placebo plus insulin group. Up to 104 weeks, minor episodes were reported in patients were 53.1% for dapagliflozin 10 mg plus insulin and 41.6% for placebo. Patients in this study could also be treated with a maximum of two oral anti-diabetes medications (OADs) including metformin.
In the dapagliflozin cardiovascular outcomes study, no increased risk of major hypoglycaemia was observed with dapagliflozin therapy compared with placebo. Major events of hypoglycaemia were reported in 58 patients (0.7%) treated with dapagliflozin and 83 (1.0%) patients treated with placebo.
Volume depletion: In the pooled analysis of 13 short-term, placebo-controlled studies, events suggestive of volume depletion (including reports of dehydration, hypovolemia or hypotension) were reported in 1.1% and 0.7% of patients who received dapagliflozin 10 mg and placebo, respectively. Across the pool of 21 active and placebo-controlled studies, serious events occurred in ≤0.2% of patients and were balanced between dapagliflozin 10 mg and comparator (see Precautions).
In the cardiovascular outcomes study, the numbers of patients with events suggestive of volume depletion were balanced between treatment groups: 213 (2.5%) and 207 (2.4%) in the dapagliflozin and placebo groups, respectively. Serious adverse events were reported in 81 (0.9%) and 70 (0.8%) in the dapagliflozin and placebo group, respectively. Events were generally balanced between treatment groups across subgroups of age, diuretic use, blood pressure and angiotensin-converting enzyme inhibitor/angiotensin receptor blocker use. In patients with eGFR <60 mL/min/1.73 m2 at baseline, there were 19 events of serious adverse events suggestive of volume depletion in 604 patients in the dapagliflozin group and 13 events in 658 patients in the placebo group.
Genital infections: In the pooled analysis of 13 short-term, placebo-controlled studies, events of genital infections were reported in 5.5% and 0.6% of patients who received dapagliflozin 10 mg and placebo, respectively. The events of genital infections reported in patients treated with dapagliflozin 10 mg were all mild to moderate. Most events of genital infection responded to an initial course of standard treatment and rarely resulted in discontinuation from the study (0.2% dapagliflozin 10 mg vs. 0% placebo). Subjects with a history of recurrent genital infection were more likely to experience an infection. Infections were more frequently reported in females (8.4% dapagliflozin 10 mg vs. 1.2% placebo) than in males (3.4% dapagliflozin 10 mg vs. 0.2% placebo). The most frequently reported genital infections were vulvovaginal mycotic infections in females, and balanitis in males.
In 9 of the 13 studies in the placebo-controlled pool, long-term data was available. In this short-term plus long-term placebo-pooled analysis (mean duration of treatment was 439.5 days for dapagliflozin 10 mg and 419.0 days for placebo); the proportions of patients with events of genital infections were 7.7% (156/2026) in the dapagliflozin 10 mg group and 1.0% (19/1956) in the placebo group. Of the patients treated with dapagliflozin 10 mg who experienced an infection, 67.9% had only one and 10.9% had 3 or more. Of the patients treated with placebo who experienced an infection, 89.5% had only one and none had 3 or more.
In the DECLARE study, the number of patients with serious adverse events of genital infections were few and balanced: 2 (<0.1%) patients in each of the dapagliflozin and placebo groups. There were 74 and 7 patients with non-serious adverse events of genital infections leading to study drug discontinuation in the dapagliflozin group and placebo group, respectively.
Necrotising fasciitis of the perineum (Fournier's gangrene): Cases of Fournier's gangrene have been reported postmarketing in patients taking SGLT2 inhibitors including dapagliflozin (see Precautions).
In the dapagliflozin cardiovascular outcome study with 17,160 type 2 diabetes mellitus patients and a median exposure time of 48 months, a total of 6 cases of Fournier's gangrene were reported, one in the dapagliflozin-treated group and 5 in the placebo group.
Urinary tract infections: In the pooled analysis of 13 short-term, placebo-controlled studies, events of urinary tract infections were reported in 4.7% and 3.5% of patients who received dapagliflozin 10 mg and placebo, respectively. Most events of urinary tract infections reported in patients treated with dapagliflozin 10 mg were mild to moderate. Most patients responded to an initial course of standard treatment, and urinary tract infections rarely caused discontinuation from the study (0.2% dapagliflozin 10 mg vs. 0.1% placebo). Subjects with a history of recurrent urinary tract infection were more likely to experience an infection. Infections were more frequently reported in females (8.5% dapagliflozin 10 mg vs. 6.7% placebo) than in males (1.8% dapagliflozin 10 mg vs. 1.3% placebo) (see Precautions).
In the short-term plus long-term placebo-pooled analysis of 9 short-term studies with long term data available, the proportions of patients with events of urinary tract infections were 8.6% in the dapagliflozin 10 mg group and 6.2% in the placebo group. Of the 59 patients treated with dapagliflozin 10 mg who experienced an infection, 77.6% had only one and 6.3% had 3 or more. Of the patients treated with placebo who experienced an infection, 77.7% had only one and 9.9% had 3 or more.
In the DECLARE study there were fewer patients with serious and adverse events of urinary tract infections in the dapagliflozin group compared with the placebo group: 79 (0.9%) and 109 (1.3%), respectively.
Diabetic ketoacidosis (DKA): In the DECLARE study with dapaglifozin in patients with type 2 diabetes, where 8574 patients received dapagliflozin 10 mg and 8569 patients received placebo, with a median exposure time of 48 months, events of DKA were reported in 27 patients in the dapagliflozin 10 mg group and 12 patients in the placebo group. The events occurred evenly distributed over the study period. Of the 27 patients with DKA events in the dapagliflozin group, 22 had concomitant insulin treatment at the time of the event. Precipitating factors for DKA were as expected in a type 2 diabetes mellitus population (see Precautions).
Events related to decreased renal function: In the 13-study, short-term, placebo-controlled pool, mean serum creatinine levels increased a small amount at Week 1 (mean change from baseline: 0.041 mg/dL dapagliflozin 10 mg versus 0.008 mg/dL placebo) and decreased toward baseline by Week 24 (mean change from baseline: 0.019 mg/dL dapagliflozin 10 mg version 0.008 mg/dL placebo). There were no further changes through Week 102.
In the cardiovascular outcomes study, there were fewer patients with marked laboratory abnormalities of creatinine, creatinine clearance, eGFR and urine albumin to creatinine ratio (UACR) in the dapagliflozin group compared with the placebo group. Fewer renal events (e.g., decreased renal creatinine clearance, renal impairment, increased blood creatinine, and decreased glomerular filtration rate) were reported in the dapaglizlofin group compared with the placebo group: 422 (4.9%) and 526 (6.1%) respectively. There were fewer patients with events reported as acute kidney injury in the dapagliflozin group compared with the placebo group: 125 (1.5%) and 175 (2.0%), respectively. There were fewer patients with SAE of renal events in the dapagliflozin group compared with the placebo group: 80 (0.9%) and 136 (1.6%), respectively. eGFR dereased over time in both treatment groups. At 1 year, mean eGFR was slightly lower, and at 4 years, mean eGFR was slightly higher in the dapagliflozin group compared with the placebo group.
Metformin hydrochloride: Metformin adverse reactions by system organ class and by frequency category.
Gastrointestinal: Very common: Mild gastrointestinal symptoms (such as diarrhoea, nausea, vomiting, abdominal pain and loss of appetite) are the most frequent reactions to metformin (>1/10), especially during the initial treatment period. These symptoms are generally transient and resolve spontaneously during continued treatment.
Occurrence of gastrointestinal symptoms, once a patient is stabilised on any dose of metformin, could be due to lactic acidosis or other serious disease.
Systemic/metabolic: Very rare: Lactic acidosis (see Precautions) is a very rare (<1/10,000) but serious metabolic complication that can occur due to metformin accumulation during treatment with metformin.
The onset of lactic acidosis is often subtle and accompanied only by non-specific symptoms such as malaise, myalgia, respiratory distress, increasing somnolence and non-specific abdominal distress. There may be associated hypothermia, hypotension and resistant bradyarrhythmias with more marked acidosis. The patient and the patient's physician must be aware of the possible importance of such symptoms and the patient should be instructed to notify the physician immediately if they occur.
Lactic acidosis should be suspected in any diabetic patient with metabolic acidosis lacking evidence of ketoacidosis (ketonuria and ketonaemia).
Lactic acidosis is a medical emergency that must be treated in hospital. In a patient with lactic acidosis who is taking metformin, the drug should be discontinued immediately and general supportive measures promptly instituted.
Nervous system disorders: Common: Taste disturbance (3%) is common.
Dermatological: Very rare: Skin reactions such as erythema, pruritus and urticaria have been reported, but the incidence is very rare (<1/10,000).
Haematological: Very rare: A decrease of vitamin B12 absorption with a decrease in serum levels has been observed in patients treated long term with metformin (<1/10,000). Consideration of such an aetiology is recommended if a patient presents with megaloblastic anaemia. Therefore, serum B12 levels should be appropriately monitored or periodic parenteral B12 supplementation considered.
Hepatobiliary disorders: Isolated reports: Liver function tests abnormalities or hepatitis resolving upon metformin discontinuation, have been reported.
In clinical trials in children and adolescents with type 2 diabetes, the profile of adverse reactions was similar to that observed in adults.
Postmarketing experience: The following postmarketing case reports have been reported during post-approval use of XIGDUO XR. Because these cases are reported voluntarily from a population of an unknown size, it is not always possible to reliably estimate their frequency.
Metabolism and nutrition disorders: Ketoacidosis.
Infections and infestations: Pyelonephritis, urosepsis, necrotising fasciitis of the perineum (Fournier's gangrene).
Skin and subcutaneous tissue disorders: Rash.
View ADR Monitoring Form